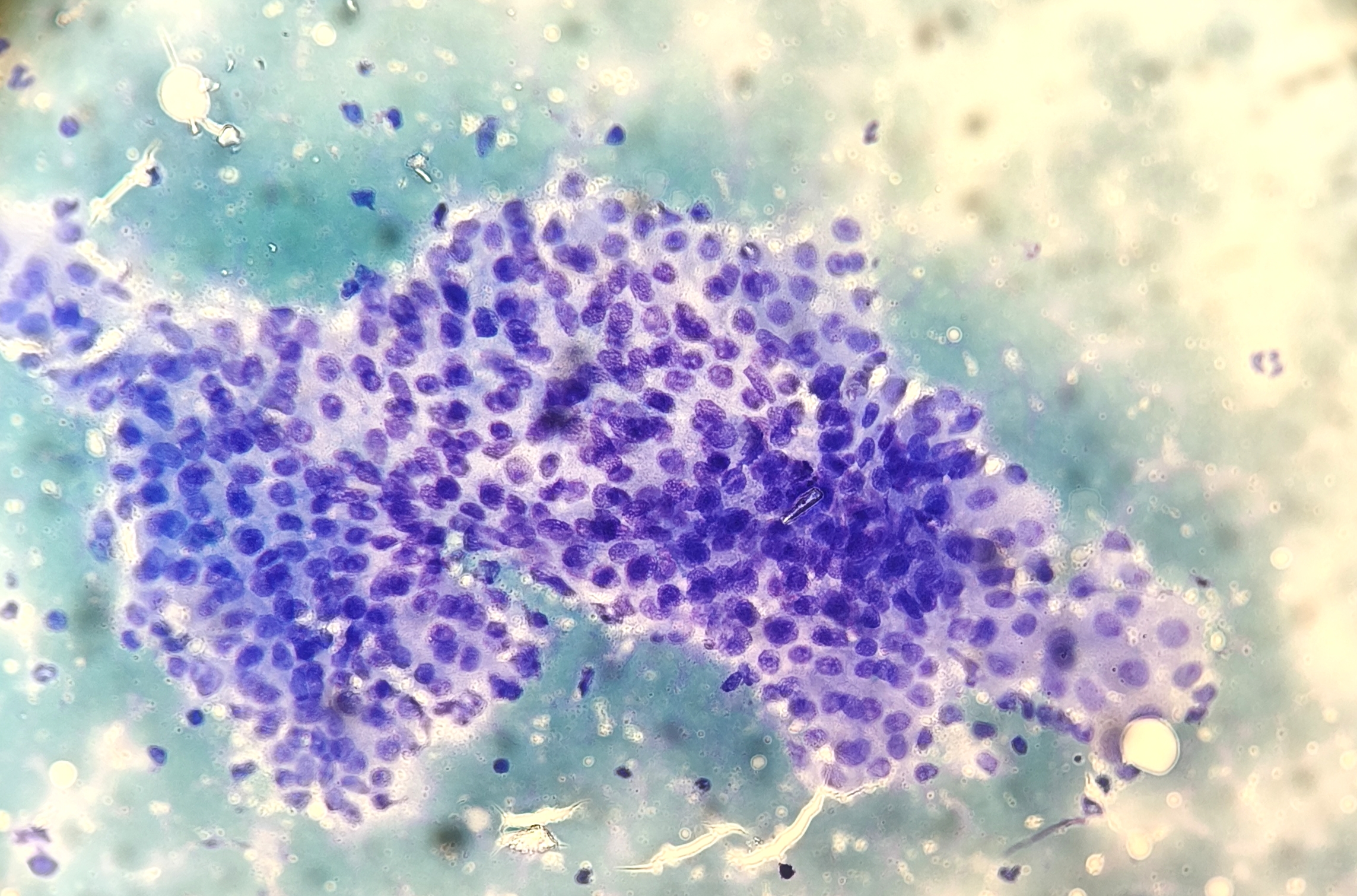
On 4 March, a 49-year-old man was referred to the Fine Needle Aspiration (FNA) Clinic at our hospital for evaluation of a large thyroid nodule. Neck ultrasound revealed a normally positioned thyroid gland with a 6 cm hypoechoic nodular mass at the isthmus. An ultrasound-guided FNA was performed in collaboration with the interventional radiology team. Two smears were prepared and immediately fixed for Papanicolaou staining.
Interview with Dr. Milagros Abad – SLAC’s president.
Nominated as SLAC since April 2017 and giving continuity to the pre-existing society of exfoliative cytology (Vienna, 1961), it is composed by 20 affiliated countries and seeks to promote the knowledge, dissemination and application of Cytopathology and the use of international and standardized reporting systems across Latin America. SLAC also counts with an official theoretical and practical exam for both, cytotechnologists and cytopathologists and every 3 years organizes a congress whose host country rotates.
This interview highlights Dr. Milagros Abad’s strategy on cytopathology education, with a vision grounded in accessibility and equity, promoting access to continuous formation, despite major economic and technological limitations in some Latin American countries.
Her tenure, focusing efforts and prioritizing global partnerships worldwide with other scientific societies in the cytology field, allowed the consolidation of major synergy projects, developing joint educational modules with a multicenter participation, in the format of co-host conferences. These collaborations elevate Latin America’s contributions on the global stage and foster a united cytology community committed to excellence. These alliances are led by the International Academy of Cytology (IAC), the ASC (American Association of Cytopathology) and the Spanish Society of Cytopathology (SEC)
The goal is to share and combine ideas, resources, knowledge and efforts to enhance the impact of the actions, while being inclusive and aligned with the dynamic nature of cytopathology, reducing disparities in access to high-quality training by promoting standardized curricula, multilingual resources, and the use of virtual platforms to reach professionals in even the most remote areas.
Virtual education has allowed SLAC to transcend geographical and economic barriers, fostering a culture of continuous learning through webinars, regional workshops, and worldwide. These digital tools ensure that education is not only accessible but also up-to-date with global standards.
Participation has grown significantly, especially among young cytopathologists and technologists who are eager for mentorship and global engagement. Scientific societies are essential pillars of advancement. They foster research, set practice standards, and provide a forum for multidisciplinary collaboration. Globally, societies like SLAC, ASC, IAC and SEC are instrumental in harmonizing diagnostic criteria, promoting quality control, and advocating for the role of cytopathology.
These results would not be possible without the teamwork and support of the entire steering SLAC committee, to whom she is deeply grateful.
Dr. Milagros Abad’s leadership reflects a deep commitment to equity, innovation, and international collaboration. Under her guidance, the Latin American Society of Cytology is not only advancing education but redefining the role of cytopathology in global health.
Dr. Milagros AbadSLAC TEAM: Drs: Esperanza Teuzaba, Analia Filippini, Rosa Laudi, Beatruz Salvagno, Milagros Abad, Ana Jaen, Carla Molina and Ana Soskin.
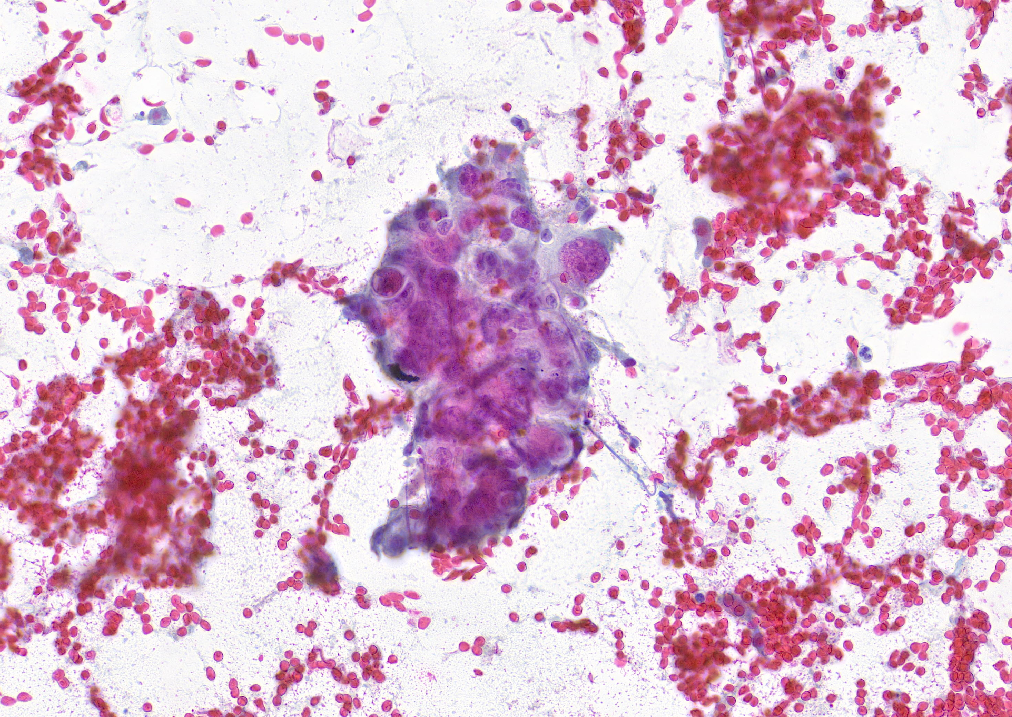
An 80-year-old male patient presented with a hypoechoic, nodular lesion of approximately 21 mm in the right parotid gland. Clinical suspicion was of a pleomorphic adenoma. Cytopathologic assessment via fine needle aspiration (FNA) was performed.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies. Cookies Policy
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.