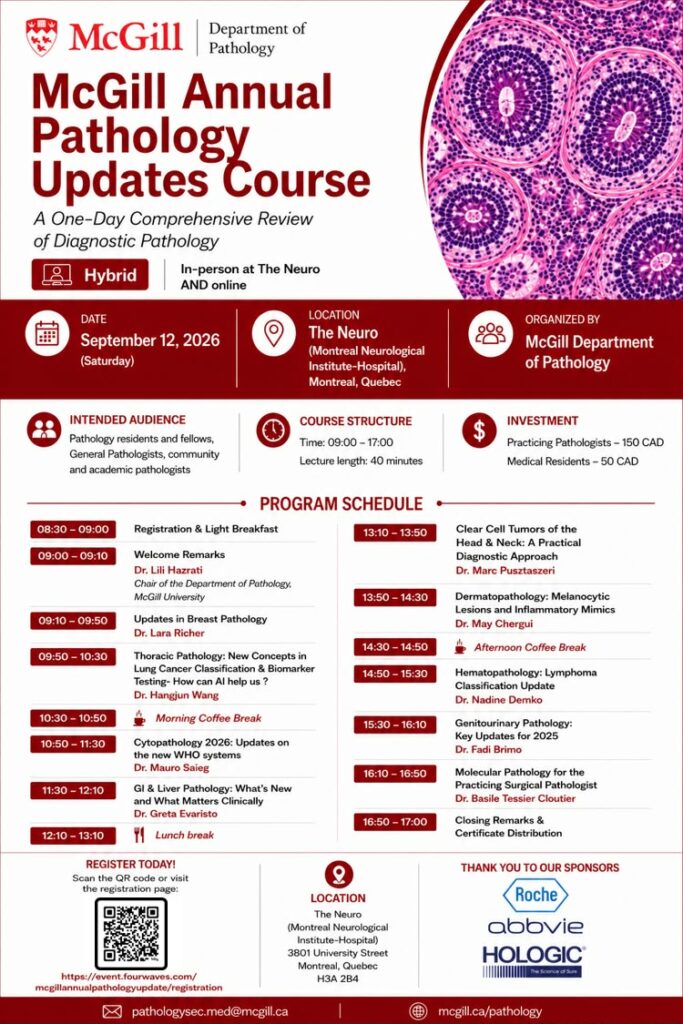
McGill Department of Pathology to Host Annual Pathology Updates Course in Montreal
The McGill Department of Pathology has announced its Annual Pathology Updates Course, a one-day comprehensive review of diagnostic pathology designed for practicing pathologists, residents, fellows, and community and academic professionals in the field.
The course will take place on Saturday, September 12, 2026, at The Neuro (Montreal Neurological Institute-Hospital) in Montreal, Quebec. In a hybrid format, participants can attend either in person or online, making the program accessible to a broader international audience.
A Full Day of Diagnostic Pathology
Running from 9:00 to 17:00, the course features a dense schedule of 40-minute lectures covering a wide range of subspecialties. After a welcome address by Dr. Lili Hazrati, Chair of the Department of Pathology at McGill University, the program moves through topics including:
- Updates in Breast Pathology (Dr. Lara Richer)
- Thoracic Pathology, including AI applications in lung cancer classification and biomarker testing (Dr. Hangjun Wang)
- Cytopathology updates on the new WHO systems (Dr. Mauro Saieg)
- GI & Liver Pathology (Dr. Greta Evaristo)
- Head & neck clear cell tumors (Dr. Marc Pusztaszeri)
- Dermatopathology: melanocytic lesions and inflammatory mimics (Dr. May Chergui)
- Hematopathology and lymphoma classification updates (Dr. Nadine Demko)
- Genitourinary Pathology updates for 2025 (Dr. Fadi Brimo)
- Molecular Pathology for the practicing surgical pathologist (Dr. Basile Tessier Cloutier)
The day includes morning and afternoon coffee breaks, a lunch break, and closing remarks with certificate distribution.
Registration and Cost
Registration is open now via QR code or online at the event page (fourwaves.com). Investment is 150 CAD for practicing pathologists and 50 CAD for medical residents.
The event is organized by the McGill Department of Pathology and sponsored by Roche, AbbVie, and Hologic.
For more information, attendees can contact pathologysec.med@mcgill.ca or visit mcgill.ca/pathology.